In this section we investigate the trends in death rates for ICD10 code I25 (Chronic ischemic heart disease), which represents 21.8% of all cardiovascular deaths in 2019 for 15 to 44 year-olds in the UK. This analysis investigates the absolute trends in adjusted deaths for a single ICD10 code. We also investigate the fraction of deaths attributable to ICD10 code I25 versus deaths from all other causes.
The methdology for establishing the baseline is described in full report.
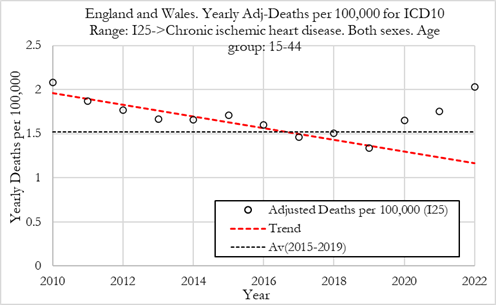
The Figures below show yearly adjusted deaths for Chronic Ischemic Heart Disease for females in England and Wales. The red dashed line shows the average from 2010 to 2019. The dotted line shows the 2015-2019 average death rate. Left: Adj-Deaths per 100,000. Right: Adj-Deaths (number).
Summary:
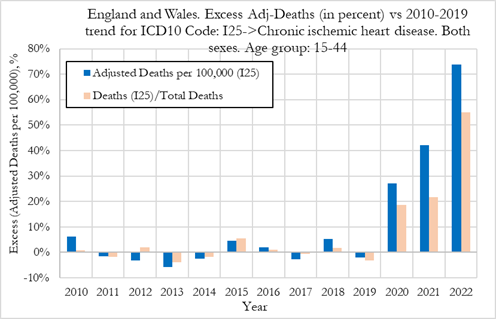
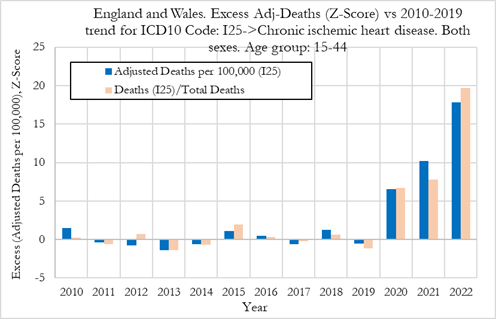
In the Figure (left) below we can observe that the excess deaths rates from chronic ischemic heart disease were +28% in 2020, then rose to about 42% in 2021 and about 74% in 2022. In terms of statistical significance of the excess deaths, we observe from Figure 10 (right) that for these cardiovascular conditions, in 2021, the Z-score for excess adjusted death rates was about 10 which points to a very strong signal (extreme event) that needs further investigating. In 2022 the Z-score rose to about 17, which is an extraordinarily strong signal and indicates that the excess deaths from chronic ischemic heart disease are statistically significant deviations from the 2010-2019 trend. We also note that in 2020, the Z-score for the excess death rates was already pointing towards a strong signal.
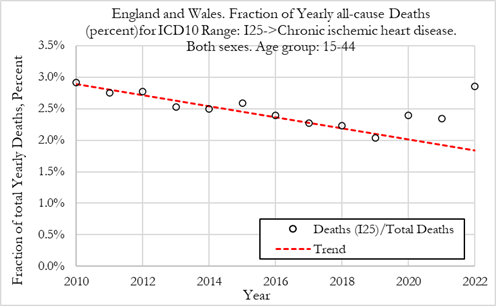
When looking at changes in the fraction of all deaths attributed to chronic ischemic heart disease, we observe that the fraction of deaths for these conditions were +18% and +22% above trend in 2020 and 2021, respectively (with a Z-score around 6, indicating high statistical significance). In 2022 however, the fraction of deaths for these conditions jumped about +55%, with a Z-score above 19 which points to a strong effect (extreme event).
Summary:
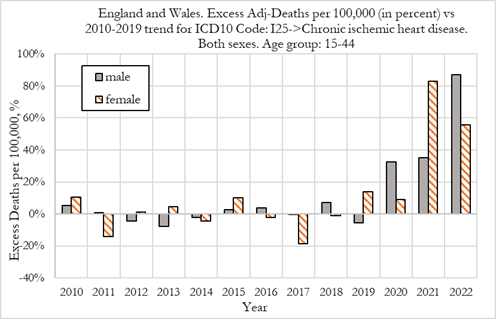
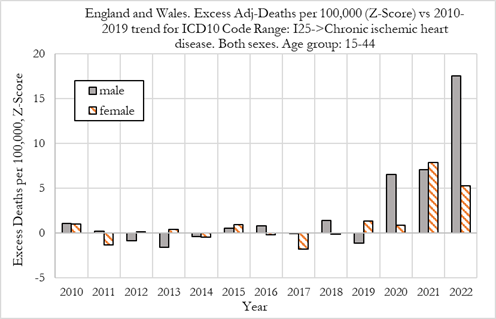
We now compare excess deaths rates from chronic ischemic heart disease for males and females aged 15-44, as shown in the Figure below.
We observe that in 2020 while female had no noticeable excess mortality (with a Z-scores below 1.0), men already experience about 33% excess mortality (with a Z-score above 6 which denotes very high statistical significance).
We also observe that in 2021 women suffered worse outcomes than men, with women experiencing a 82% deviation from trend, compared to about 36% for men. These values are strong signals, with Z-scores above 6.
In 2022, men suffered worse outcomes than women, with men experiencing about 86% deviation from trend, compared to about 56% for women. The signal strength for men was very strong (with a Z-score of close to 18) and for women the signal was also very strong signals (albeit with a lower Z-score of about 5), as shown in Figure (right).
Summary:
In this section we investigate the trends in death rates for ICD10 code I21 (Acute Myocardial infarction), which represents 18.2% of all cardiovascular deaths in 2019 for 15 to 44 year-olds in the UK. This analysis investigates the absolute trends in adjusted deaths for a single ICD10 code. We also investigate the fraction of deaths attributable to ICD10 code I21 versus deaths from all other causes.
The methdology for establishing the baseline is described in full report.
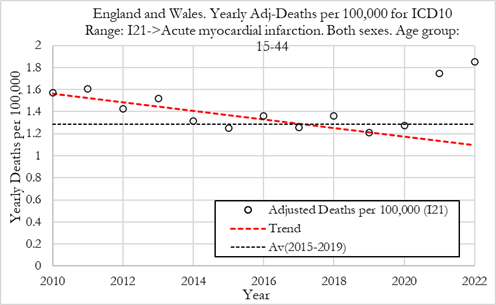
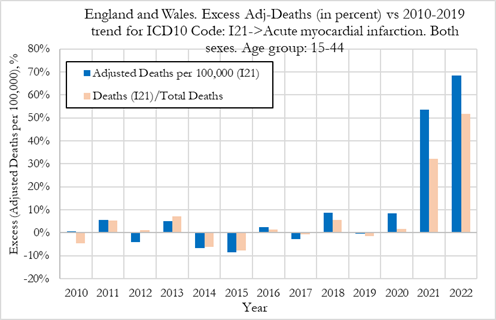
The Figures below show yearly adjusted deaths from acute myocardial infarction in England and Wales. The red dashed line shows the average from 2010 to 2019. The dotted line shows the 2015-2019 average death rate. Left: Adj-Deaths per 100,000. Right: Adj-Deaths (number).
Summary:
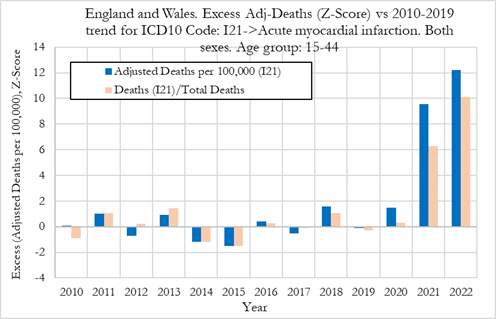
In the Figure (left) below we can observe that the excess deaths rates from acute myocardial infarction were +9% in 2020, then jumped to about 53% in 2021 and about 69% in 2022. In terms of statistical significance of the excess deaths, we observe from Figure (right) that for these cardiovascular conditions, in 2020, the Z-score for excess adjusted death rates was below 2 which points to a low statistical significance (within normal bounds). In 2021 however, the Z-score for excess adjusted death rates was about to 9.5 which points to a very strong signal (extreme event). In 2022 the Z-score rose to about 12, which is an extraordinarily strong signal and indicates that the excess deaths from acute myocardial infarction are statistically significant deviations from the 2010-2019 trend.
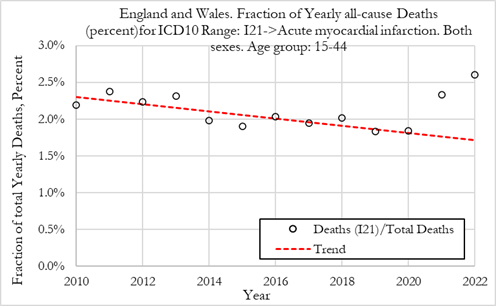
When looking at changes in the fraction of all deaths attributed to acute myocardial infarction, we observe that the fraction of deaths for these conditions were only +1% above trend in 2020, with a Z-score close to 0 showing no statistical significance. In 2021 and 2022 however, the fraction of deaths for these conditions jumped about +31% and +51% with Z-scores around 6 and 10, respectively pointing to a strong effect (extreme event).
Summary:
When looking at deaths attributed to acute myocardial infarction for males and females, shown in Figure 14, we observe that in 2020 there was a +6% excess mortality for men and +20% for women. For men the excess mortality was not a signal, with respective Z-scores of about 1.5 (low statistical significance). However, for women, the rise in excess mortality could be seen as a weak signal (with Z-score around 2) which would warrant further investigation.
In 2021 men and women suffered similar outcomes, with men experiencing a 52% deviation from trend, compared to about 66% for women. These values, constitute very strong signals, as the Z-score was around 6.0 for women and close to 10 for men.
In 2022 men suffered much worse outcomes than women, with men experiencing about 82% deviation from trend, compared to about 50% for women. The signal strength for men was very strong (with a Z-score above 15) but for women the signal was still strong albeit weaker than in 2021 (with a Z-score above 4), as shown in Figure 14-right.
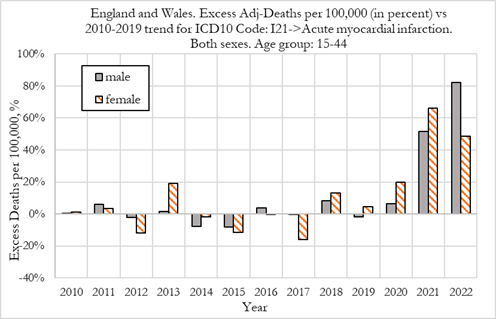
We now compare excess deaths rates from acute myocardial infarction for males and females aged 15-44, as shown in the Figure below.
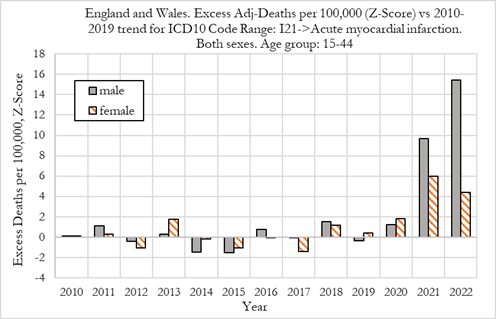
We observe that in 2020 there was a +6% excess mortality for men and +20% for women. For men the excess mortality was not a signal, with respective Z-scores of about 1.5 (low statistical significance). However, for women, the rise in excess mortality could be seen as a weak signal (with Z-score around 2) which would warrant further investigation.
In 2021 men and women suffered similar outcomes, with men experiencing a 52% deviation from trend, compared to about 66% for women. These values, constitute very strong signals, as the Z-score was around 6.0 for women and close to 10 for men.
In 2022 men suffered much worse outcomes than women, with men experiencing about 82% deviation from trend, compared to about 50% for women. The signal strength for men was very strong (with a Z-score above 15) but for women the signal was still strong albeit weaker than in 2021 (with a Z-score above 4), as shown in Figure (right).
Summary:
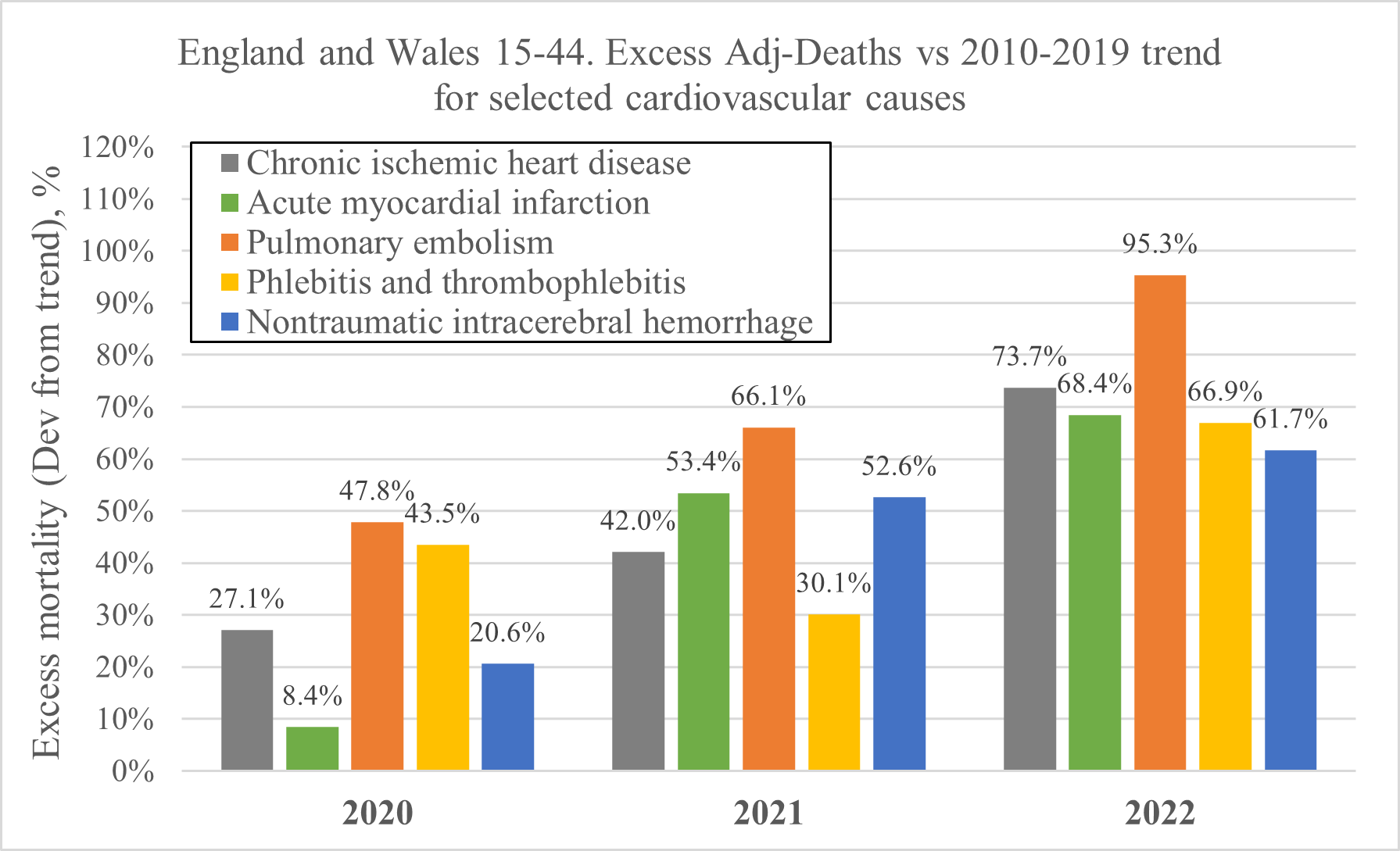
The chart below shows an overview of the excess mortality for selected cardiovascular events, which are analysed in detail in the full report.

 PHINANCE TECHNOLOGIES
PHINANCE TECHNOLOGIES